
What is follicular lymphoma?
Follicular lymphoma is the second most frequent type of non-Hodgkin’s lymphoma, accounting for 20-25% of all non-Hodgkin’s lymphomas. Around 2,000 new cases are diagnosed each year in Spain. It is a type B lymphoma and slow-growing (indolent), although some follicular lymphomas can grow rapidly.
The average age of diagnosis of people with follicular lymphoma is about 60 years, being rare in young people. It usually affects many lymphatic areas of the body as well as the bone marrow.
Follicular lymphoma originates in the germinal centre B-cells. The germinal centres occur in the secondary lymphoid organs (e.g. spleen or lymph nodes) and this is where the B-cells mature, differentiate and proliferate. In about 25-35% of patients with follicular lymphoma, the disease transforms to a high-grade (aggressive) lymphoma, usually diffuse large B-cell lymphoma (DLBCL) See diffuse large B-cell lymphoma.
The causes of this type of lymphoma are unknown, and with respect to symptomatology, it is not uncommon for it to be diagnosed in asymptomatic individuals in whom imaging or laboratory tests are performed for other reasons
In follicular NHL, examination of the biopsy of a lymph node may reveal different histological subtypes:
– Small cell predominant (Grade 1),
– Mixed small and large cell pattern (Grade 2) and
– Large cell predominant (Grade 3).
The main interest of this classification is that grade 3 lymphomas with a predominance of large cells, called centroblasts, have a progression and prognosis closer to diffuse large B-cell lymphomas See diffuse large B-cell lymphoma. and should be managed as such.
The histological study should always be completed with an immunohistochemical, cytogenetic (mostly presenting translocation 14,18) and molecular study to have perfectly typed lymphoma and to make a correct differential diagnosis with other very similar lymphomas.
What is the treatment for follicular lymphoma?
 There is currently no “standard” treatment for follicular lymphoma. The doctor will assess an individual diagnosis, the stage and grade of the lymphoma, as well as age and general health before deciding what treatment is appropriate.
There is currently no “standard” treatment for follicular lymphoma. The doctor will assess an individual diagnosis, the stage and grade of the lymphoma, as well as age and general health before deciding what treatment is appropriate.
Stage I and II follicular lymphomas:
In very localised cases, with lesions less than 7.5 cm in diameter, radiotherapy as a sole treatment might be indicated as this may be curative.
If not localised, close monitoring of the patient’s condition by cautious waiting rather than active treatment administration is possible. As with other chronic or slow-onset diseases, the uncertainty of living with them with monitoring but without treatment can be emotionally challenging for patients. Therefore, it is always advisable to consult with your haematologist or appropriate patient associations in order to access emotional support if deemed necessary. See useful links.
Stage III or IV follicular lymphomas:
Induction therapy is recommended with the aim of shrinking the tumours, followed by maintenance therapy which increases the chance of cure (called complete remission) as well as the duration of remission (since the tendency of this lymphoma to recur must be taken into account). The most common induction therapy is a monoclonal antibody targeting CD20 expressed on the lymphoma cells (Rituximab or Obinutuzumab) combined with chemotherapy, usually a CHOP-type schedule (cyclophosphamide, adriamycin, vincristine and prednisone), up to 8 cycles, every 21 days, or alternatively bendamustine with rituximab, up to 6 cycles, every 28 days.
Maintenance therapy begins after completion of induction therapy and consists of Rituximab every 2 months for 2 years.

Treatment of relapses
Relapse of disease means that the disease recurs (at the same or different site), after response to and completion of initial treatment. Depending on the time between completion of treatment and recurrence, and the type of treatment given before, there are several effective options available, including chemotherapy, Rituximab, radioimmunotherapy and stem cell transplantation. Thus, the options are:
- Rituximab or, if it has been used before, obinotuzumab with bendamustine
- Rituximab-CHOP chemotherapy (cyclophosphamide, doxorubicin, vincristine, prednisone) or with CVP (cyclophosphamide, vincristine, prednisone), if Rituximab and bendamustine have been used before.
- Chemotherapy Rituximab – ESHAP (Etoposide, Prednisolone, Cytarabine and Cisplatin, of choice in patients in whom a subsequent autologous transplant is planned.

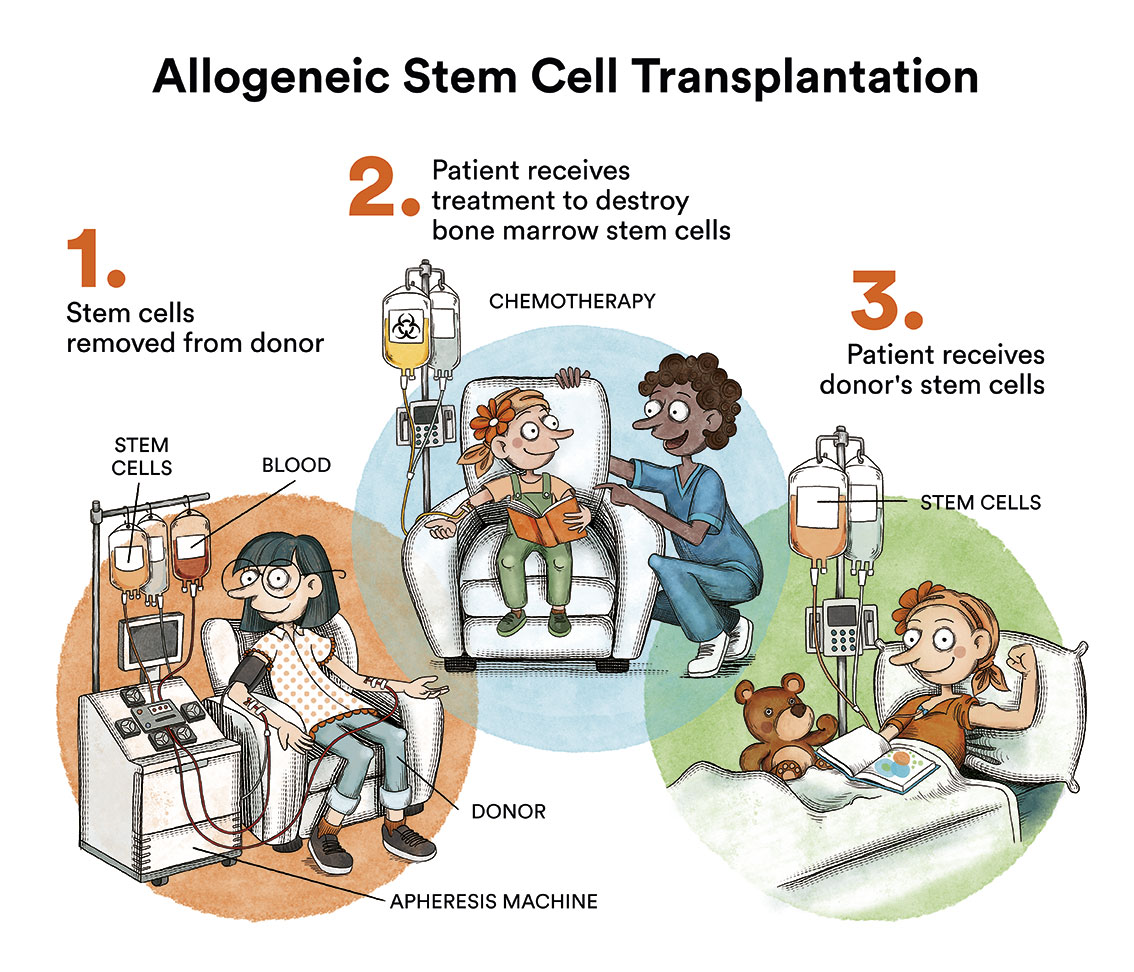
The autologous stem cell transplant is thus envisaged as consolidation of response in patients up to 70 years of age without comorbidities, while the allogeneic transplant (donor) is usually reserved for relapses after autologous transplantation. Nowadays, with the emergence of new immunotherapy strategies, the latter is an increasingly infrequent indication.
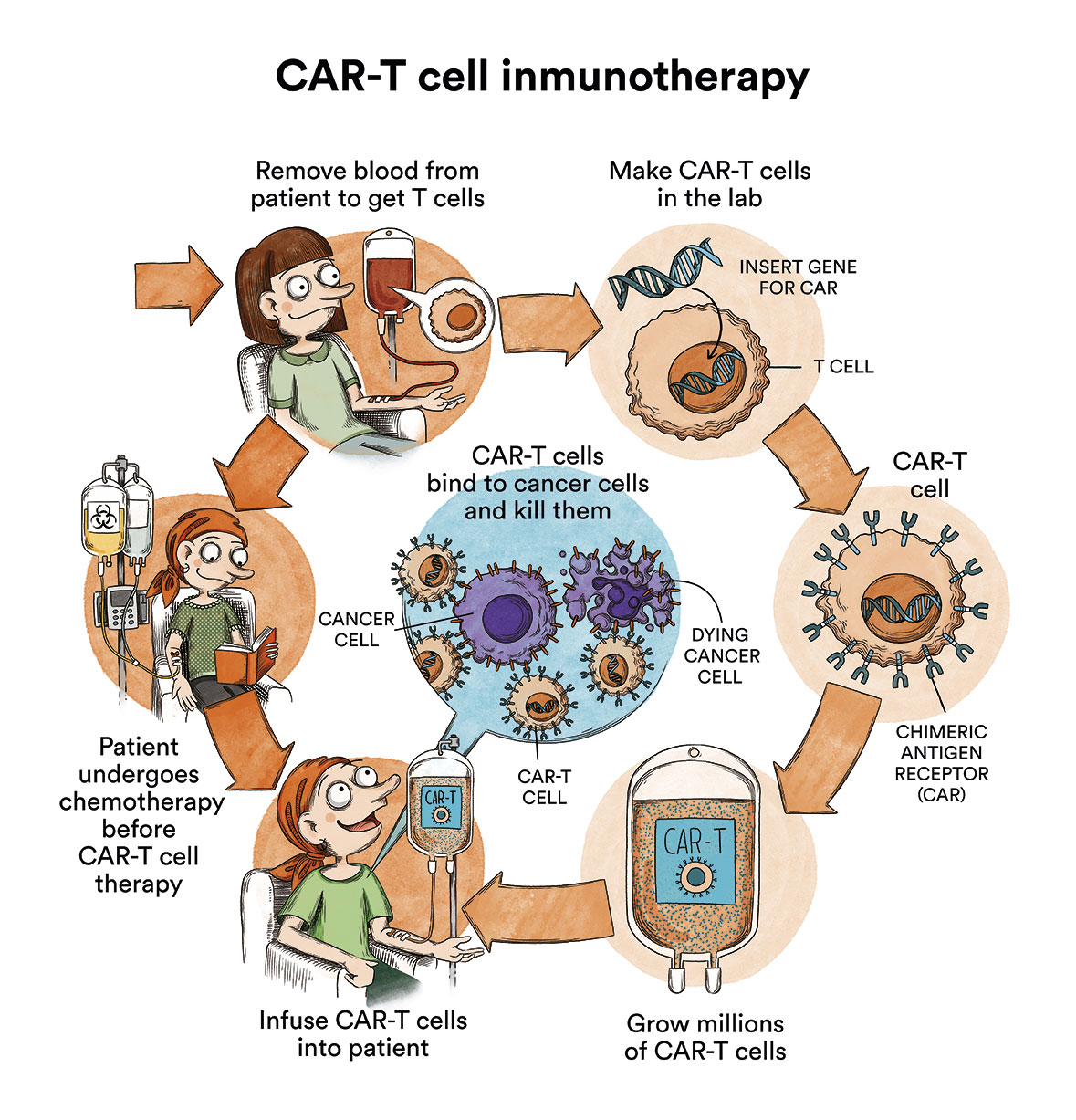
The role of immunotherapy with the bi-specific monoclonal antibodies or the CART cell therapy (content in spanish) (therapies targeting specific lymphoma markers) is currently growing with promising results. While CART is contemplated for transformed follicular lymphomas that have received at least 2 prior lines of therapy, or are primarily refractory, they are usually used within clinical trials. A treatment clinical trial is a research study aimed at improving current treatments or obtaining information on new treatments for cancer patients.
What are the chances of patients with follicular lymphoma being cured?
Follicular lymphomas usually respond very well to available treatments, but are difficult to cure. Their natural history is characterised by a pattern of continuous relapses and a high sensitivity to chemotherapy that decreases over successive relapses.
Therefore, depending on a number of prognostic factors, these lymphomas may not require treatment when diagnosed and treatment may be delayed until the lymphoma starts to cause problems. Over time, some follicular lymphomas may develop into diffuse large B-cell lymphoma and will be treated as such.
In an attempt to predict the outcome of follicular lymphomas, the impact of a number of prognostic factors such as age, number of lymphoid areas involved, bone marrow involvement, haemoglobin values (presence of anaemia) and LDH values (tumour growth marker) have been analysed.
The prognostic index using these variables is called FLIPI and based on this index patients can be classified as low, intermediate, or high risk, with very different survival rates. However, this index should be considered as an indicative tool as it was established before the availability of the new immunochemotherapy agents (IQT) that have completely changed the probability of survival of these patients, who have now reached median survival times of up to 20 years.
Other factors of notable impact are the duration of response to the first treatment (less than one year: worse prognosis) and transformation to high-grade lymphoma (worse prognosis).
Links of interest concerning medical issues relating to follicular lymphoma
Follicular lymphoma. Blood Cancer UK
Follicular lymphoma. Cancer Research UK
Follicular lymphoma. Macmillan Cancer Support
Links of interest on other topics related to non-Hodgkin’s lymphoma:
TESTIMONIAL MATERIALS
You can order the booklets in paper format for free delivery in Spain by e-mail: imparables@fcarreras.es
BONE MARROW TRANSPLANT
- Bone Marrow Transplant Guide. Josep Carreras Foundation (content in Spanish)
- What is HLA and how does it work? Josep Carreras Foundation (content in Spanish)
- Graft-versus-Host Disease. Josep Carreras Foundation (content in Spanish)
- History of Bone Marrow Transplantation. Josep Carreras Foundation (content in Spanish)
- How is the search for an anonymous donor conducted? Josep Carreras Foundation (content in Spanish)
FOOD
- How to maintain a healthy diet during treatment? Josep Carreras Foundation (content in Spanish)
- Nutrition guide. Leukemia & Lymphoma Society
OTHER
- Ideas on what to take with me to the isolation chamber. Josep Carreras Leukaemia Foundation (content in Spanish)
- Travel tips for people with cancer. Josep Carreras Leukaemia Foundation (content in Spanish)
- Physiotherapy manual for haematological and transplant patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Prevention and treatment of oral mucositis. Josep Carreras Leukaemia Foundation (content in Spanish)
- Oral hygiene in oncohaematological patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Fertility manual: Suffering from blood cancer and becoming a parent. Josep Carreras Leukaemia Foundation (content in Spanish)
- Skin care in the oncohaematological patient. Josep Carreras Leukaemia Foundation (content in Spanish)
- Aesthetic Oncology Manual. Josep Carreras Leukaemia Foundation (content in Spanish)
- Leukaemia and sexuality. Josep Carreras Leukaemia Foundation (content in Spanish)
- 7 ways to wear a scarf. Josep Carreras Leukaemia Foundation (content in Spanish)
Links of interest: local/provincial or state entities that can provide you with resources and services specialised in leukaemia, lymphoma or cancer patients:
In Spain there is a large network of associations for haematological cancer patients which, in many cases, can provide information, advice and even carry out certain procedures. These are the contacts of some of them by Autonomous Community:
All these organisations are external to the Josep Carreras Foundation.
STATE
- AMILO (Asociación Española de Amiloidosis)
- ACLIF (Asociación para la cura del linfoma folicular)
- AEAL (ASOCIACIÓN ESPAÑOLA DE AFECTADOS POR LINFOMA, MIELOMA y LEUCEMIA)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch or call al 900 100 036 (24h).
- AELCLES (Agrupación Española contra la Leucemia y Enfermedades de la Sangre)
- CEMMP (Comunidad Española de Pacientes de Mieloma Múltiple)
- JoSEP CARRERAS LEUKAEMIA FOUNDATION
- FUNDACIÓN SANDRA IBARRA
- GEPAC (GRUPO ESPAÑOL DE PACIENTES CON CÁNCER)
- MPN España (Asociación de Afectados Por Neoplasias Mieloproliferativas Crónicas)
ANDALUCÍA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ALUSVI (ASOCIACIÓN LUCHA Y SONRÍE POR LA VIDA). Sevilla
- APOLEU (ASOCIACIÓN DE APOYO A PACIENTES Y FAMILIARES DE LEUCEMIA). Cádiz
ARAGÓN
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASPHER (ASOCIACIÓN DE PACIENTES DE ENFERMEDADES HEMATOLÓGICAS RARAS DE ARAGÓN)
- DONA MÉDULA ARAGÓN
ASTURIAS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASTHEHA (ASOCIACIÓN DE TRASPLANTADOS HEMATOPOYÉTICOS Y ENFERMOS HEMATOLÓGICOS DE ASTURIAS)
CANTABRIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LA MANCHA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LEÓN
- ABACES (ASOCIACIÓN BERCIANA DE AYUDA CONTRA LAS ENFERMEDADES DE LA SANGRE)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ALCLES (ASOCIACIÓN LEONESA CON LAS ENFERMEDADES DE LA SANGRE). León.
- ASCOL (ASOCIACIÓN CONTRA LA LEUCEMIA Y ENFERMEDADES DE LA SANGRE). Salamanca.
CATALUÑA
- ASSOCIACIÓ FÈNIX. Solsona
- FECEC (FEDERACIÓ CATALANA D’ENTITATS CONTRA EL CÁNCER
- FUNDACIÓ KÁLIDA. Barcelona
- FUNDACIÓ ROSES CONTRA EL CÀNCER. Roses
- LLIGA CONTRA EL CÀNCER COMARQUES DE TARRAGONA I TERRES DE L’EBRE. Tarragona
- MielomaCAT
- ONCOLLIGA BARCELONA. Barcelona
- ONCOLLIGA GIRONA. Girona
- ONCOLLIGA COMARQUES DE LLEIDA. Lleida
- ONCOVALLÈS. Vallès Oriental
- OSONA CONTRA EL CÀNCER. Osona
- SUPORT I COMPANYIA. Barcelona
- VILASSAR DE DALT CONTRA EL CÀNCER. Vilassar de Dalt
VALENCIAN COMMUNITY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASLEUVAL (ASOCIACIÓN DE PACIENTES DE LEUCEMIA, LINFOMA, MIELOMA Y OTRAS ENFERMEDADES DE LA SANGRE DE VALENCIA)
EXTREMADURA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AFAL (AYUDA A FAMILIAS AFECTADAS DE LEUCEMIAS, LINFOMAS; MIELOMAS Y APLASIAS)
- AOEX (ASOCIACIÓN ONCOLÓGICA EXTREMEÑA)
GALICIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASOTRAME (ASOCIACIÓN GALLEGA DE AFECTADOS POR TRASPLANTES MEDULARES)
BALEARIC ISLANDS
- ADAA (ASSOCIACIÓ D’AJUDA A L’ACOMPANYAMENT DEL MALALT DE LES ILLES BALEARS)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CANARY ISLANDS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AFOL (ASOCIACIÓN DE FAMILIAS ONCOHEMATOLÓGICAS DE LANZAROTE)
- FUNDACIÓN ALEJANDRO DA SILVA
LA RIOJA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
MADRID
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AEAL (ASOCIACIÓN ESPAÑOLA DE LEUCEMIA Y LINFOMA)
- CRIS CONTRA EL CÁNCER
- FUNDACIÓN LEUCEMIA Y LINFOMA
MURCIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
NAVARRA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
BASQUE COUNTRY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- PAUSOZ-PAUSO. Bilbao
AUTONOMOUS CITIES OF CEUTA AND MELILLA
- AECC CEUTA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
- AECC MELILLA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
Support and assistance
We also invite you to follow us through our main social media (Facebook, Twitter and Instagram) where we often share testimonies of overcoming this disease.
If you live in Spain, you can also contact us by sending an e-mail to imparables@fcarreras.es so that we can help you get in touch with other people who have overcome this disease.