
What is mantle cell lymphoma?
 A mantle cell lymphoma (MCL) is a rare type of aggressive B-cell non-Hodgkin’s lymphoma that accounts for about 10% of all non-Hodgkin’s lymphomas. It occurs in older people and is more common in males. Half of the patients are older than 65 years at diagnosis. It usually involves the bone marrow, lymph nodes, spleen and the digestive tract, including the oesophagus, stomach and intestines. Mantle cell lymphoma (MCL) is characterised by a genetic change within the lymphoma cells involving chromosomes 11 and 14. This genetic change alters the function of a protein called cyclin D1. Some patients have a slower growing form of the disease. In these cases a period of surveillance without treatment is usually recommended until signs of damage or disease progression appear.
A mantle cell lymphoma (MCL) is a rare type of aggressive B-cell non-Hodgkin’s lymphoma that accounts for about 10% of all non-Hodgkin’s lymphomas. It occurs in older people and is more common in males. Half of the patients are older than 65 years at diagnosis. It usually involves the bone marrow, lymph nodes, spleen and the digestive tract, including the oesophagus, stomach and intestines. Mantle cell lymphoma (MCL) is characterised by a genetic change within the lymphoma cells involving chromosomes 11 and 14. This genetic change alters the function of a protein called cyclin D1. Some patients have a slower growing form of the disease. In these cases a period of surveillance without treatment is usually recommended until signs of damage or disease progression appear.
There are two variants of the disease: the common or classic type and blast variant, which is more aggressive and difficult to treat.
The causes of mantle cell lymphoma (MCL) are currently unknown. It is neither an infectious nor an inherited disease, there are no environmental factors that are clearly related to its development.
In MCL, the disease is usually at an advanced stage at diagnosis. The patient may present with the general B symptoms of lymphomas (night sweats, fever, weight loss) and usually splenomegaly (enlargement of a lymph node). Extranodal involvement is very frequent (90% of patients), especially invasion of the bone marrow and gastrointestinal tract.
Histological study of the biopsied lymph node or tissue should always be completed by immunohistochemical, cytogenetic and molecular study. In the case of MCL, the typical chromosomal translocation (11,14), involving increased expression of cyclin D1 within the cells, must be demonstrated, which is essential for differential diagnosis with other similar lymphomas. A number of secondary chromosomal alterations may also be present. Ki-67 staining is useful to assess the proliferative activity of this type of tumour.
How is mantle cell lymphoma treated?
Mantle cell lymphoma is often a type of lymphoma that does not respond well to long-term treatment.
For this reason, it is important that haematologists use the Mantle Cell Lymphoma International Prognostic Index (MIPI) which lists the clinical factors that most influence the prognosis of this type of lymphoma. The MIPI takes into account four factors at the time of diagnosis that are independent of each other and are scored from 0 to 3 depending on whether or not they are altered:
- the patient’s age
- the patient’s general condition
- the level of lactate dehydrogenase (LDH) in the blood
- the leukocyte (white blood cell) count in the blood
This will allow a prognosis to be established for the patient’s tolerance to chemotherapy. The MIPI assigns a low risk (0 to 3 points), intermediate risk or high risk (6 to 11 points) category to the patient.
The treatment of choice for mantle cell lymphoma is chemotherapy (which can be associated with radiotherapy (on localised or large affected areas according to the schemes detailed below:

– The scheme called R-CHOP, which associates rituximab with cyclophosphamide, adriamycin, vincristine and prednisone, generally alternated with R-DHAP (rituximab, dexamethasone, cytarabine and cisplatin), a total of 6 cycles.
– Rituximab associated with Hyper-CVAD (cyclophosphamide, vincristine, doxorubicin [Adriamycin] and dexamethasone) alternating with high doses of methotrexate and cytarabine.
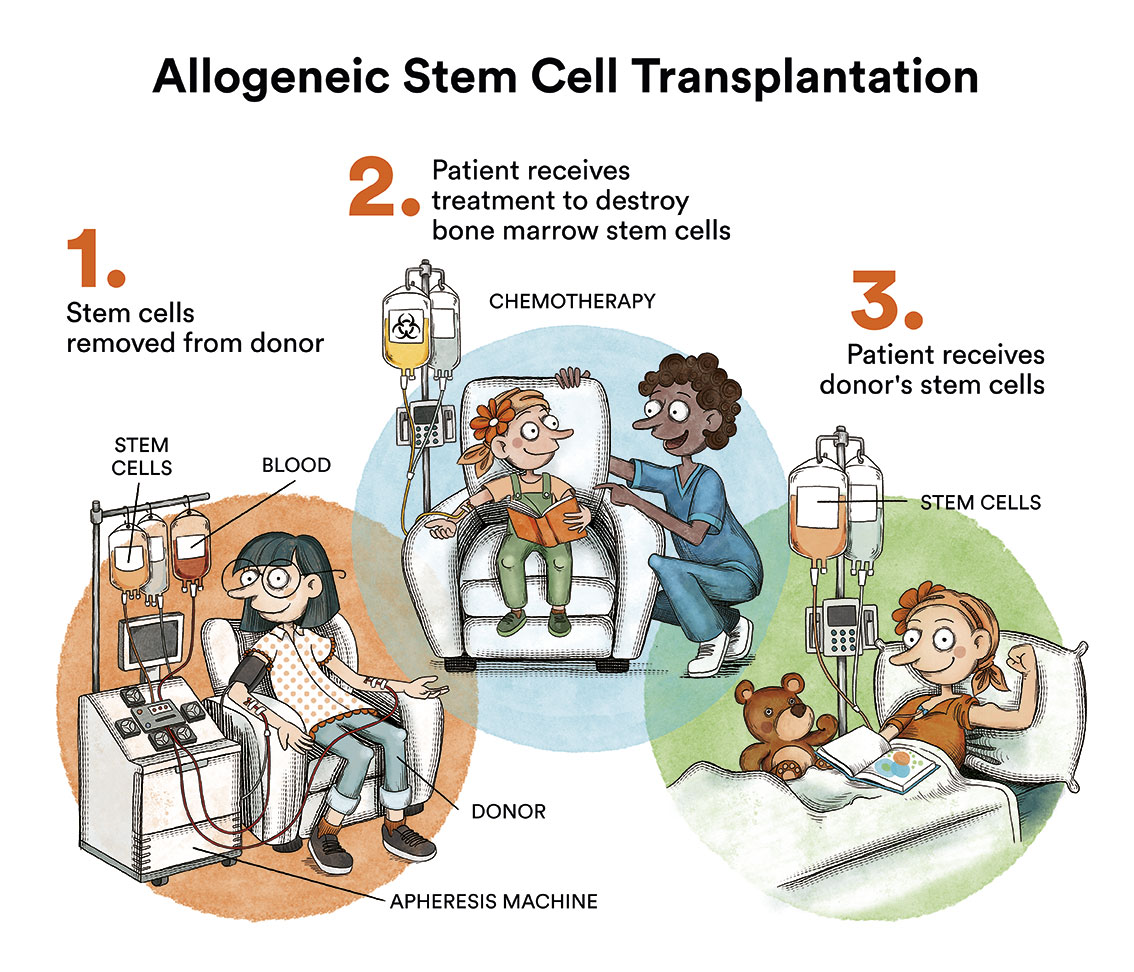
– In young patients, up to 65-70 years of age, and without comorbidities and with chemosensitive disease, an autologous haematopoietic stem cell transplant is proposed as consolidation therapy, which has been shown to improve the duration of disease response rate and overall survival. After transplantation, maintenance treatment with rituximab is recommended every 2 months for 3 years
– In patients who are not transplant candidates, the two most commonly used regimens are R-CHOP (usually up to 6 cycles, followed by maintenance Rituximab every 2 months indefinitely) and R-Bendamustine.
The allogeneic haematopoietic stem cell transplantation is reserved for young patients (<70 years) with an available donor, in good health, who have relapsed after an autologous transplant, and provided that the disease responds to salvage therapy (that it is chemosensitive).
In patients refractory to first-line treatment or relapsed, provided the disease remains chemosensitive, other treatment options may include:
– Targeted drugs such as ibrutinib (Imbruvica®), acalabrutinib (Calquence®), zanubrutinib (Brukinsa®), bortezomib (Velcade®), venetoclax (Venclexta®). Of these, ibrutinib, which is generally associated with rituximab, offers the best efficacy and toxicity profile and has an approved indication in this disease.
– Chemotherapy (with drugs other than those initially used, such as gemcitabine or bendamustine with cytarabine), often in combination with rituximab.
– Drugs from immunotherapy such as lenalidomide (Revlimid®) together with rituximab.
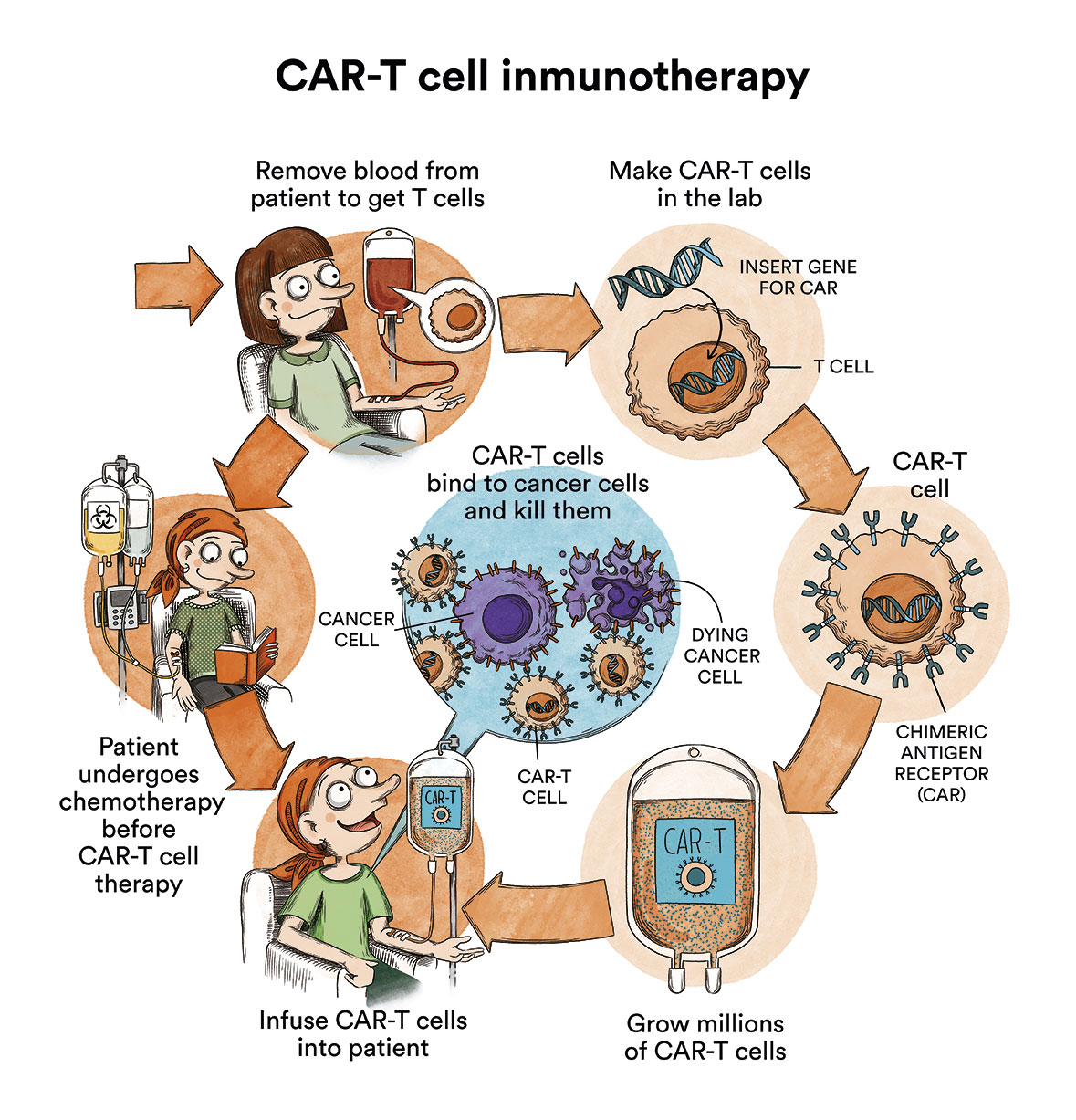
– CAR-T cell therapy with brexucel (Tercatus), specific therapy for primary refractory or relapsed mantle lymphoma after or without prior autologous transplantation beyond the first complete remission. It is administered only in national tertiary centres that have been authorised by the Ministry of Health, and each case must be assessed and approved by a national expert committee
For older patients with mantle cell lymphoma who are in poor health, less intensive approaches are the best option to control the disease without causing relevant toxicities or harm with treatment.
What are the chances of patients with mantle cell lymphoma being cured?
Research in recent years offers many more therapeutic opportunities for these patients. However, although most patients respond well to the first lines of treatment, relapses are very common. The median duration of remission, according to most studies, is 1.5 to 3 years. The prognosis for the blast variant of mantle cell lymphoma is less favourable. However, new, more targeted immunotherapy treatments are currently being tested and are likely to lead to an improved prognosis in the coming years. Bone marrow transplantation from a compatible donor (allogeneic transplantation) is currently the only curative option for these patients.
Links of interest concerning medical issues relating to mantle cell lymphoma
Mantle Cell Lymphoma Facts. Leukamia & Lymphoma Foundation
Mantle cell lymphoma. Cancer Research UK
Mantle cell lymphoma. Macmillan Cancer Support
Links of interest on other topics related to non-Hodgkin’s lymphoma:
TESTIMONIAL MATERIALS
You can order the booklets in paper format for free delivery in Spain by e-mail: imparables@fcarreras.es
BONE MARROW TRANSPLANT
- Bone Marrow Transplant Guide. Josep Carreras Foundation (content in Spanish)
- What is HLA and how does it work? Josep Carreras Foundation (content in Spanish)
- Graft-versus-Host Disease. Josep Carreras Foundation (content in Spanish)
- History of Bone Marrow Transplantation. Josep Carreras Foundation (content in Spanish)
- How is the search for an anonymous donor conducted? Josep Carreras Foundation (content in Spanish)
FOOD
- How to maintain a healthy diet during treatment? Josep Carreras Foundation (content in Spanish)
- Nutrition guide. Leukemia & Lymphoma Society
OTHER
- Ideas on what to take with me to the isolation chamber. Josep Carreras Leukaemia Foundation (content in Spanish)
- Travel tips for people with cancer. Josep Carreras Leukaemia Foundation (content in Spanish)
- Physiotherapy manual for haematological and transplant patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Prevention and treatment of oral mucositis. Josep Carreras Leukaemia Foundation (content in Spanish)
- Oral hygiene in oncohaematological patients. Josep Carreras Leukaemia Foundation (content in Spanish)
- Fertility manual: Suffering from blood cancer and becoming a parent. Josep Carreras Leukaemia Foundation (content in Spanish)
- Skin care in the oncohaematological patient. Josep Carreras Leukaemia Foundation (content in Spanish)
- Aesthetic Oncology Manual. Josep Carreras Leukaemia Foundation (content in Spanish)
- Leukaemia and sexuality. Josep Carreras Leukaemia Foundation (content in Spanish)
- 7 ways to wear a scarf. Josep Carreras Leukaemia Foundation (content in Spanish)
Links of interest: local/provincial or state entities that can provide you with resources and services specialised in leukaemia, lymphoma or cancer patients:
In Spain there is a large network of associations for haematological cancer patients which, in many cases, can provide information, advice and even carry out certain procedures. These are the contacts of some of them by Autonomous Community:
All these organisations are external to the Josep Carreras Foundation.
STATE
- AMILO (Asociación Española de Amiloidosis)
- ACLIF (Asociación para la cura del linfoma folicular)
- AEAL (ASOCIACIÓN ESPAÑOLA DE AFECTADOS POR LINFOMA, MIELOMA y LEUCEMIA)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch or call 900 100 036 (24h).
- AELCLES (Agrupación Española contra la Leucemia y Enfermedades de la Sangre)
- CEMMP (Comunidad Española de Pacientes de Mieloma Múltiple)
- JOSEP CARRERAS LEUKAEMIA FOUNDATION
- FUNDACIÓN SANDRA IBARRA
- GEPAC (GRUPO ESPAÑOL DE PACIENTES CON CÁNCER)
- MPN España (Asociación de Afectados Por Neoplasias Mieloproliferativas Crónicas)
ANDALUCÍA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ALUSVI (ASOCIACIÓN LUCHA Y SONRÍE POR LA VIDA). Sevilla
- APOLEU (ASOCIACIÓN DE APOYO A PACIENTES Y FAMILIARES DE LEUCEMIA). Cádiz
ARAGÓN
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASPHER (ASOCIACIÓN DE PACIENTES DE ENFERMEDADES HEMATOLÓGICAS RARAS DE ARAGÓN)
- DONA MÉDULA ARAGÓN
ASTURIAS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASTHEHA (ASOCIACIÓN DE TRASPLANTADOS HEMATOPOYÉTICOS Y ENFERMOS HEMATOLÓGICOS DE ASTURIAS)
CANTABRIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LA MANCHA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CASTILLA LEÓN
- ABACES (ASOCIACIÓN BERCIANA DE AYUDA CONTRA LAS ENFERMEDADES DE LA SANGRE)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ALCLES (ASOCIACIÓN LEONESA CON LAS ENFERMEDADES DE LA SANGRE). León.
- ASCOL (ASOCIACIÓN CONTRA LA LEUCEMIA Y ENFERMEDADES DE LA SANGRE). Salamanca.
CATALUÑA
- ASSOCIACIÓ FÈNIX. Solsona
- FECEC (FEDERACIÓ CATALANA D’ENTITATS CONTRA EL CÁNCER
- FUNDACIÓ KÁLIDA. Barcelona
- FUNDACIÓ ROSES CONTRA EL CÀNCER. Roses
- LLIGA CONTRA EL CÀNCER COMARQUES DE TARRAGONA I TERRES DE L’EBRE. Tarragona
- MielomaCAT
- ONCOLLIGA BARCELONA. Barcelona
- ONCOLLIGA GIRONA. Girona
- ONCOLLIGA COMARQUES DE LLEIDA. Lleida
- ONCOVALLÈS. Vallès Oriental
- OSONA CONTRA EL CÀNCER. Osona
- SUPORT I COMPANYIA. Barcelona
- VILASSAR DE DALT CONTRA EL CÀNCER. Vilassar de Dalt
VALENCIAN COMMUNITY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASLEUVAL (ASOCIACIÓN DE PACIENTES DE LEUCEMIA, LINFOMA, MIELOMA Y OTRAS ENFERMEDADES DE LA SANGRE DE VALENCIA)
EXTREMADURA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AFAL (AYUDA A FAMILIAS AFECTADAS DE LEUCEMIAS, LINFOMAS; MIELOMAS Y APLASIAS)
- AOEX (ASOCIACIÓN ONCOLÓGICA EXTREMEÑA)
GALICIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- ASOTRAME (ASOCIACIÓN GALLEGA DE AFECTADOS POR TRASPLANTES MEDULARES)
BALEARIC ISLANDS
- ADAA (ASSOCIACIÓ D’AJUDA A L’ACOMPANYAMENT DEL MALALT DE LES ILLES BALEARS)
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
CANARY ISLANDS
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AFOL (ASOCIACIÓN DE FAMILIAS ONCOHEMATOLÓGICAS DE LANZAROTE)
- FUNDACIÓN ALEJANDRO DA SILVA
LA RIOJA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
MADRID
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- AEAL (ASOCIACIÓN ESPAÑOLA DE LEUCEMIA Y LINFOMA)
- CRIS CONTRA EL CÁNCER
- FUNDACIÓN LEUCEMIA Y LINFOMA
MURCIA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
NAVARRA
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
BASQUE COUNTRY
- AECC (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER). Present in the different provinces and in many municipalities. Contact the nearest branch.
- PAUSOZ-PAUSO. Bilbao
AUTONOMOUS CITIES OF CEUTA AND MELILLA
- AECC CEUTA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
- AECC MELILLA (ASOCIACIÓN ESPAÑOLA CONTRA EL CÁNCER)
Support and assistance
We also invite you to follow us through our main social media (Facebook, Twitter and Instagram) where we often share testimonies of overcoming this disease.
If you live in Spain, you can also contact us by sending an e-mail to imparables@fcarreras.es so that we can help you get in touch with other people who have overcome this disease.